
MONO-1
JADE MONO-1 and MONO-2 were two identically designed double-blind pivotal phase 3 monotherapy studies that evaluated the efficacy and safety of CIBINQO without Rx topicals vs placebo in patients with moderate to severe AD.1
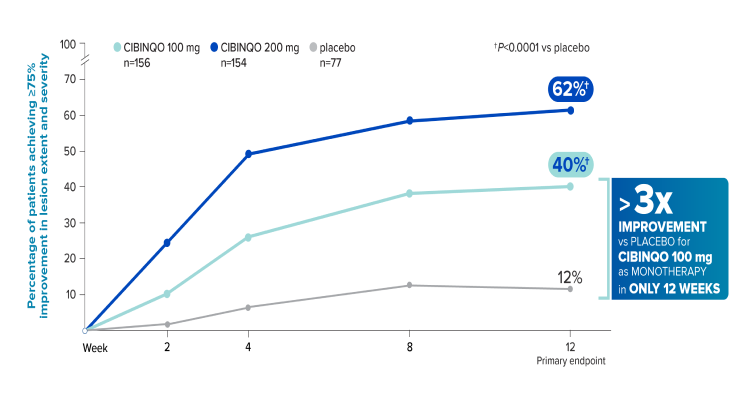
Powerful skin clearance results without TCS1,2*

JADE MONO-1: EASI-75 for CIBINQO 100 mg or 200 mg vs placebo (co-primary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
IGA response 0/1 at week 12 (co-primary endpoint): 24% of patients taking CIBINQO 100 mg (P<0.01 vs placebo), 44% taking CIBINQO 200 mg (P<0.0001 vs placebo), and 8% taking placebo achieved IGA 0/1.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication. All missing responses were defined as non-responders.
A responder was defined as achieving IGA 0 or 1 and at least a 2-point improvement from baseline.
*Patients were permitted to use nonmedicated emollients during the study.
EASI-75=≥75% improvement in lesion extent and severity from baseline on the Eczema Area and Severity Index; IGA=Investigator's Global Assessment; TCS=topical corticosteroids.
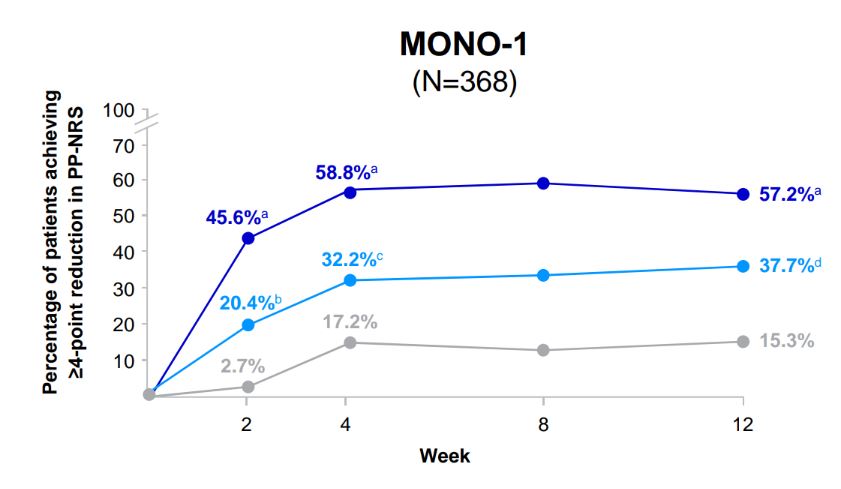
Rapid and significant itch relief without TCS1,2*
JADE MONO-1: PP-NRS4 for CIBINQO 100 mg or 200 mg vs placebo (key secondary endpoint)

The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
A higher proportion of patients treated with CIBINQO 100 mg or 200 mg achieved improvement in itching at week 12 vs placebo.§
§Based on PSAAD at week 12.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication.
All missing responses were defined as non-responders.
*Patients were permitted to use nonmedicated emollients during the study.
PP-NRS4=≥4-point reduction from baseline on the Peak Pruritus Numerical Rating Scale; PSAAD=Pruritus and Symptoms Assessment for Atopic Dermatitis; TCS=topical corticosteroids.
Powerful skin clearance results without TCS1,2*
JADE MONO-1: EASI-75 for CIBINQO 100 mg or 200 mg vs placebo (co-primary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
IGA response 0/1 at week 12 (co-primary endpoint): 24% of patients taking CIBINQO 100 mg (P<0.01 vs placebo), 44% taking CIBINQO 200 mg (P<0.0001 vs placebo), and 8% taking placebo achieved IGA 0/1.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication. All missing responses were defined as non-responders.
A responder was defined as achieving IGA 0 or 1 and at least a 2-point improvement from baseline.
*Patients were permitted to use nonmedicated emollients during the study.
EASI-75=≥75% improvement in lesion extent and severity from baseline on the Eczema Area and Severity Index; IGA=Investigator's Global Assessment; TCS=topical corticosteroids.
Rapid and significant itch relief without TCS1,2*
JADE MONO-1: PP-NRS4 for CIBINQO 100 mg or 200 mg vs placebo (key secondary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
A higher proportion of patients treated with CIBINQO 100 mg or 200 mg achieved improvement in itching at week 12 vs placebo.§
§Based on PSAAD at week 12.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication.
All missing responses were defined as non-responders.
*Patients were permitted to use nonmedicated emollients during the study.
PP-NRS4=≥4-point reduction from baseline on the Peak Pruritus Numerical Rating Scale; PSAAD=Pruritus and Symptoms Assessment for Atopic Dermatitis; TCS=topical corticosteroids.
MONO-2
Powerful skin clearance results without TCS1,2*
JADE MONO-2: EASI-75 for CIBINQO 100 mg or 200 mg vs placebo (co-primary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
IGA response 0/1 at week 12 (co-primary endpoint): 28% of patients taking CIBINQO 100 mg (P<0.001 vs placebo), 38% taking CIBINQO 200 mg (P<0.0001 vs placebo), and 9% taking placebo achieved IGA 0/1.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication. All missing responses were defined as non-responders.
A responder was defined as achieving IGA 0 or 1 and at least a 2-point improvement from baseline.
*Patients were permitted to use nonmedicated emollients during the study.
EASI-75=≥75% improvement in lesion extent and severity from baseline on the Eczema Area and Severity Index; IGA=Investigator's Global Assessment; TCS=topical corticosteroids.
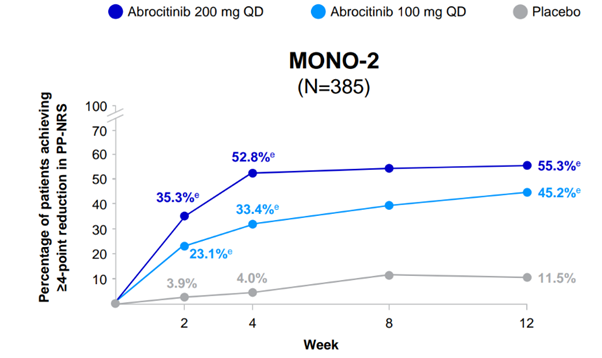
Rapid and significant itch relief without TCS1,2*
JADE MONO-2: PP-NRS4 for CIBINQO 100 mg or 200 mg vs placebo (key secondary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
A higher proportion of patients treated with CIBINQO 100 mg or 200 mg achieved improvement in itching at week 12 vs placebo.§
§Based on PSAAD at week 12.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication.
All missing responses were defined as non-responders.
*Patients were permitted to use nonmedicated emollients during the study.
PP-NRS4=≥4-point reduction from baseline on the Peak Pruritus Numerical Rating Scale; PSAAD=Pruritus and Symptoms Assessment for Atopic Dermatitis; TCS=topical corticosteroids.
Powerful skin clearance results without TCS1,2*
JADE MONO-2: EASI-75 for CIBINQO 100 mg or 200 mg vs placebo (co-primary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
IGA response 0/1 at week 12 (co-primary endpoint): 28% of patients taking CIBINQO 100 mg (P<0.001 vs placebo), 38% taking CIBINQO 200 mg (P<0.0001 vs placebo), and 9% taking placebo achieved IGA 0/1.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication. All missing responses were defined as non-responders.
A responder was defined as achieving IGA 0 or 1 and at least a 2-point improvement from baseline.
*Patients were permitted to use nonmedicated emollients during the study.
EASI-75=≥75% improvement in lesion extent and severity from baseline on the Eczema Area and Severity Index; IGA=Investigator's Global Assessment; TCS=topical corticosteroids.
Rapid and significant itch relief without TCS1,2*
JADE MONO-2: PP-NRS4 for CIBINQO 100 mg or 200 mg vs placebo (key secondary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
A higher proportion of patients treated with CIBINQO 100 mg or 200 mg achieved improvement in itching at week 12 vs placebo.§
§Based on PSAAD at week 12.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication.
All missing responses were defined as non-responders.
*Patients were permitted to use nonmedicated emollients during the study.
PP-NRS4=≥4-point reduction from baseline on the Peak Pruritus Numerical Rating Scale; PSAAD=Pruritus and Symptoms Assessment for Atopic Dermatitis; TCS=topical corticosteroids.
Study design1,2
JADE MONO-1 and MONO-2 were two identically designed double-blind pivotal phase 3 monotherapy studies that evaluated the efficacy and safety of CIBINQO without Rx topicals vs placebo in patients with moderate to severe AD.
- Co-primary endpoints:
- EASI-75 response at week 12 vs placebo
- IGA 0/1 response with ≥2-point improvement at week 12 vs placebo
- Key secondary endpoints:
- PP-NRS4 response at weeks 2, 4, and 12 vs placebo
- PSAAD response at week 12 vs placebo
In the JADE clinical trial program, EASI and IGA excluded scalp, palms, and soles from the assessment/scoring.
† At week 12, eligible subjects entered the long-term extension study (JADE EXTEND).
AD=atopic dermatitis; EASI-75=≥75% improvement in lesion extent and severity from baseline on the Eczema Area and Severity Index; IGA=Investigator’s Global Assessment; PP-NRS4=≥4-point reduction from baseline on the Peak Pruritus Numerical Rating Scale; PSAAD=Pruritus and Symptoms Assessment for Atopic Dermatitis.
JADE MONO-2 baseline characteristic 2-4
The baseline characteristics were similar for JADE MONO-1.
* Plus–minus values are means ± SD. Percentages may not total 100 because of rounding.
† Race was reported by the patients.
‡ Scores on EASI range from 0 to 72, with higher scores indicating more severe disease.
§
Scores on PP-NRS represent maximum itch severity in the previous 24 hours and range from 0 to 10, with higher scores representing more severe itch.
SD=standard deviation; BMI=body mass index; IGA=Investigator’s Global Assessment; EASI=Eczema Area and Severity Index; BSA=body surface area; PP-NRS=Peak Pruritus Numerical Rating Scale.
JADE MONO-2 baseline characteristic 2-4
The baseline characteristics were similar for JADE MONO-1.
* Plus–minus values are means ± SD. Percentages may not total 100 because of rounding.
† Race was reported by the patients.
‡ Scores on EASI range from 0 to 72, with higher scores indicating more severe disease.
§
Scores on PP-NRS represent maximum itch severity in the previous 24 hours and range from 0 to 10, with higher scores representing more severe itch.
SD=standard deviation; BMI=body mass index; IGA=Investigator’s Global Assessment; EASI=Eczema Area and Severity Index; BSA=body surface area; PP-NRS=Peak Pruritus Numerical Rating Scale.
JADE MONO-1 and MONO-2 Inclusion/exclusion criteria2-3
- Inclusion criteria
- ≥12 years of age
- Body weight ≥88 lbs
- Clinically diagnosed with chronic AD for ≥1 year, confirmed by the Hanifin and Rajka criteria of AD at the screening and baseline visits*
- Have a documented history of inadequate response to previous topical therapy, or were subjects for whom topical treatments were medically inadvisable, or require systemic therapies to control their disease
- Moderate-to-severe AD defined as BSA ≥10%, IGA ≥3, EASI ≥16, and PP-NRS ≥4 at the baseline visit
- Exclusion criteria
- Active forms of other inflammatory skin diseases
- Prior treatment with any JAK inhibitors
- Vaccination with, or exposure to, a live or attenuated vaccine within 6 weeks prior to the first dose
- Participation in other clinical studies involving investigational drug(s) within 8 weeks prior to study entry
- Uncontrolled, clinically significant laboratory abnormality that could affect study interpretation
- Any major psychiatric condition
- Unwillingness to discontinue current AD medications prior to the study
- Requiring treatment with prohibited medications during the study
- Medical history of thrombocytopenia, coagulopathy or platelet dysfunction, or Q wave interval abnormalities
- Presence or history of certain infections, cancers, lymphoproliferative disorders, and other medical conditions at the discretion of the investigator
- Pregnant or breastfeeding women
- Women of childbearing potential who are unwilling to use contraception
* Criteria include ≥3 of the basic features of pruritus; typical morphology and distribution, including flexural lichenification or linearity in adults and facial and extensor involvement in infants and children; chronic or chronically relapsing dermatitis; and personal or family history of atopy (asthma, allergic rhinitis, atopic dermatitis); along with ≥3 of 23 minor features specified in the criteria.
JAK=Janus kinase.
JADE MONO-1 and MONO-2 Inclusion/exclusion criteria2-3
- Inclusion criteria
- ≥12 years of age
- Body weight ≥88 lbs
- Clinically diagnosed with chronic AD for ≥1 year, confirmed by the Hanifin and Rajka criteria of AD at the screening and baseline visits*
- Have a documented history of inadequate response to previous topical therapy, or were subjects for whom topical treatments were medically inadvisable, or require systemic therapies to control their disease
- Moderate-to-severe AD defined as BSA ≥10%, IGA ≥3, EASI ≥16, and PP-NRS ≥4 at the baseline visit
- Exclusion criteria
- Active forms of other inflammatory skin diseases
- Prior treatment with any JAK inhibitors
- Vaccination with, or exposure to, a live or attenuated vaccine within 6 weeks prior to the first dose
- Participation in other clinical studies involving investigational drug(s) within 8 weeks prior to study entry
- Uncontrolled, clinically significant laboratory abnormality that could affect study interpretation
- Any major psychiatric condition
- Unwillingness to discontinue current AD medications prior to the study
- Requiring treatment with prohibited medications during the study
- Medical history of thrombocytopenia, coagulopathy or platelet dysfunction, or Q wave interval abnormalities
- Presence or history of certain infections, cancers, lymphoproliferative disorders, and other medical conditions at the discretion of the investigator
- Pregnant or breastfeeding women
- Women of childbearing potential who are unwilling to use contraception
* Criteria include ≥3 of the basic features of pruritus; typical morphology and distribution, including flexural lichenification or linearity in adults and facial and extensor involvement in infants and children; chronic or chronically relapsing dermatitis; and personal or family history of atopy (asthma, allergic rhinitis, atopic dermatitis); along with ≥3 of 23 minor features specified in the criteria.
JAK=Janus kinase.
References:
- Cibinqo (abrocitinib) latest approved Isareli prescribing information.
- Data on file. Pfizer Inc; New York, NY.
- Silverberg JI, Simpson EL, Thyssen JP, et al. Efficacy and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2020;156(8):863-873. doi:10.1001/jamadermatol.2020.1406.
- Simpson EL, Sinclair R, Forman S, et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): a multicentre, double-blind, randomized, placebo-controlled, phase 3 trial. Lancet. 2020;396(10246):255-266.
- Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Dermatovener (Stockholm). 1980;92(suppl):44-47.
Powerful skin clearance results without TCS1,2*
JADE MONO-1: EASI-75 for CIBINQO 100 mg or 200 mg vs placebo (co-primary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
IGA response 0/1 at week 12 (co-primary endpoint): 24% of patients taking CIBINQO 100 mg (P<0.01 vs placebo), 44% taking CIBINQO 200 mg (P<0.0001 vs placebo), and 8% taking placebo achieved IGA 0/1.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication. All missing responses were defined as non-responders.
A responder was defined as achieving IGA 0 or 1 and at least a 2-point improvement from baseline.
*Patients were permitted to use nonmedicated emollients during the study.
EASI-75=≥75% improvement in lesion extent and severity from baseline on the Eczema Area and Severity Index; IGA=Investigator's Global Assessment; TCS=topical corticosteroids.
Powerful skin clearance results without TCS1,2*
JADE MONO-1: EASI-75 for CIBINQO 100 mg or 200 mg vs placebo (co-primary endpoint)
The recommended starting dose is CIBINQO 200 mg once daily
- A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age and in patients at high risk for DVT/PE.
For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 in the LPD. - During treatment, the dose may be decreased or increased based on tolerability and efficacy.
The lowest effective dose for maintenance should be considered.
The maximum daily dose is 200 mg. - Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks.
IGA response 0/1 at week 12 (co-primary endpoint): 24% of patients taking CIBINQO 100 mg (P<0.01 vs placebo), 44% taking CIBINQO 200 mg (P<0.0001 vs placebo), and 8% taking placebo achieved IGA 0/1.
Full Analysis Set (FAS) was defined as all randomized subjects who received at least one dose of study medication. All missing responses were defined as non-responders.
A responder was defined as achieving IGA 0 or 1 and at least a 2-point improvement from baseline.
*Patients were permitted to use nonmedicated emollients during the study.
EASI-75=≥75% improvement in lesion extent and severity from baseline on the Eczema Area and Severity Index; IGA=Investigator's Global Assessment; TCS=topical corticosteroids.